

Disease elimination is the holy grail of public health, a goal rarely achieved and often difficult to maintain.
The eradication of smallpox globally, and the elimination of polio in much of the world, for example, has saved millions of lives. In contrast, measles and malaria continue to kill and maim, despite huge efforts to fight these scourges.
Remarkably, today, Ireland stands on the brink of eliminating another disease – the blood-borne virus, hepatitis C – but only if thousands of carriers are properly identified and treated.
Thanks to the development of wonder drugs that can treat the disease within weeks, without any major side effects, the elimination of hepatitis C within a decade is a possibility.
Indeed, so confident is Ireland of achieving this goal that we have signed up to the World Health Organisation target to get rid of the disease by 2030.
Yet doctors and patient groups are warning that chance could be squandered if the Health Service Executive fails to ramp up and transform its treatment programme to meet the needs of patients.
Contrasting Ireland’s approach to the radical steps taken in other countries (see panel), they say hepatitis C will continue to plague Ireland for decades unless a new approach is adopted.
The HSE rejects this criticism and says it is confident the WHO target will be met.
So which side is right? Is Ireland doing all it can to meet the WHO target? Or will patients die unnecessarily because available, affordable treatments are not extended to them?
Affordability
In other challenges within the health service, the problem often lies with the affordability or efficacy of treatments. But with hepatitis C, the challenge is that most of the patients have not been diagnosed, because many are unaware they have it.
Hepatitis C, often dubbed the “silent killer”, is a virus that infects the liver. For years, the sufferer may feel nothing only tiredness but, left untreated, it goes on to cause cirrhosis and liver cancer.
The history of hepatitis C in Ireland is coloured by the scandal that saw 1,700 people, mostly women, infected by State-supplied blood products in the 1970s and 1990s. Fixing that mess has cost €1.5 billion so far, with the bills still coming in.
Not surprisingly, when new drugs were developed to treat the disease, successive governments jumped at the chance to right historical wrongs by curing infected patients. But early treatments were hugely expensive, had horrendous side effects and produced mixed results.
In this decade, though, new drugs have come on the market that are easy to take – in tablet form – much cheaper and have far higher success rates.
Since 2015, the Department of Health has allocated €30 million a year to fund the Irish treatment programme.
With time, yet more drugs were developed and it became possible to treat more patients with the available money. Success rates rose to over 95 per cent. By the end of 2017, all State-infected patients had been successfully treated.
At this point, however, the nature of the challenge fundamentally changed. The "low-hanging fruit", to use Fine Gael TD Kate O'Connell's phrase, had been plucked, as State-infected patients were cured in the eight hospitals providing treatment.
Slow to engage
In contrast, the vast majority of people who still have hepatitis C are drug users, who often lead chaotic lives and are slow to engage with the hospital system.
While the HSE says Ireland is still on track to get rid of the disease, others are not so sure.
"We were the first to sign up to the WHO target, but we may be the last country to reach it," says Prof Jack Lambert an infectious diseases consultant at the Mater hospital. "This is not something to be proud of."
In one hospital project, he says, just two out of 40 drug-users invited to undergo treatment managed to complete the course of medication
"We are failing to in community services. Scotland invested £15 million to strengthen the community and is treating 2,500 people per year. We have invested nothing and we are on track to enrol 1,100, down from 1,700 last year.
“People from this community are very suspicious of secondary [hospital] care,” says GP Austin O’Carroll, whose work in Dublin’s north inner city brings him into regular contact with drug-users and the homeless. “If you get them at the point of contact [with services in the community] it works far better.”
In one hospital project, he says, just two out of 40 drug-users invited to undergo treatment managed to complete the course of medication.
Ireland’s systems aren’t set up to allow GPs or community pharmacies to prescribe the medication, he points out.
Five years
Prof Aiden McCormick, clinical director of the national hepatitis C programme, is confident Ireland is on track to eliminate the disease. “We’re going to make hepatitis C a rare diagnosis before 2030, and under budget,” he tells The Irish Times “The way we’re going, we’ll have it done in five years.”
Prof McCormick adumbrates the efforts made to extend the programme by offering services in nine community locations over the past two years.
He acknowledges the delays that have arisen with the provision of extra staff to test prisoners (“bogged down in interviews”) and to allow community GPs to prescribe hepatitis C drugs (“ran foul of regulations”).
The issue of numbers divides the two sides. Critics of the programme cite estimates of the hepatitis C population of between 20,000 and 30,000, but Prof McCormick believes the real number of people infected is much lower. The numbers affected have been “inflated”, he says, in part through “double-counting” of patients.
“There’s less of it than we think,” he says, adding that infection rates are declining due to reduced needle use and lower than expected figures among immigrants.
Money, he insists, is not an issue; although last year’s budget was not fully spent “we can treat as many patients as are found”.
The price of treatment has dropped by a factor of 10 since they were introduced, and now stands at about €10,000 per patient. With this cost likely to fall further as more drugs are developed and existing ones go off patent, allowing generics to come forward, the enthusiasm of pharmaceutical companies for large-scale programmes to treat patients in the short terms becomes easier to understand.

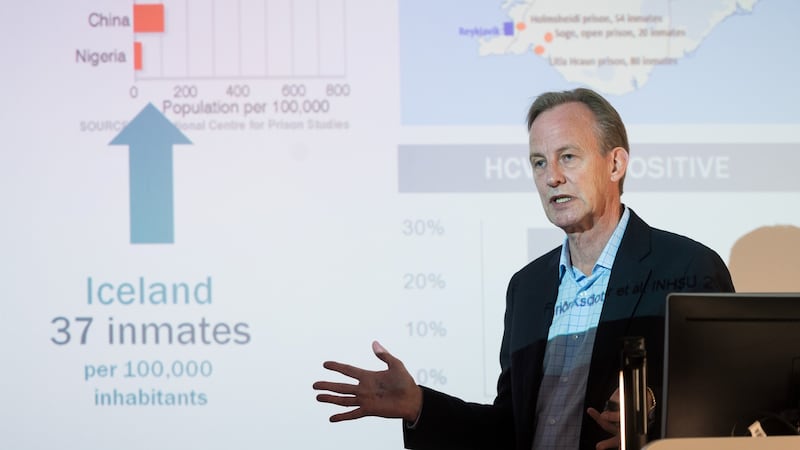
THE ICELANDIC EXPERIENCE
Iceland is on track to be one of the first countries in the world to eliminate hepatitis C, thanks to a muscular approach to screening, harm reduction among drug-users, and the provision of treatment in the community rather than hospital settings.
The Nordic nation is often put forward as a role model for the approach Ireland could take in tackling the elimination of hepatitis C in the hard-to-reach populations.
In both countries, the majority of cases are found among drug-users, with overlaps to the prison and homeless populations. The numbers involved in Iceland are far smaller than in Ireland, though.
"We target those who are most likely to spread the disease. We try to maximise the number of patients accepting treatment and compliance with the treatment, and we aim to minimise reinfections," says Heidi Fridriksdottir, manager of the Treatment as Prevention for Hepatitis C in Iceland programme.
“Many of our patients never see a doctor. You can’t give them an appointment and expect them to turn up,” she explains. Instead, under the programme, health workers actively seek out potential patients in the community – in homeless shelters, prisons and needle exchanges, for example.
Testing regimes are reduced to a minimum and delays have been ironed out so that people found to be carrying hepatitis C can be treated within weeks. “We have treated people out of the back of a car and it’s been no problem.”
To maximise the number of cases identified, screening in emergency departments has been increased and an opt-out system for screening of prisoners has been introduced.
Health workers use social media to communicate with patients, and incentives are offered to encourage compliance with treatment. These include taxi pickups, mobile phone minutes and vouchers of increasing value during the treatment course.
Drug-users are provided with harm reduction boxes containing needles and syringes, and even tourniquets to facilitate injection. “You have to get out on the street, build up trust and your street cred. We build a net around each patient to keep them in the system,” says Fridriksdottir.
The results have been dramatic; of 800 people treated, 633 have been completely cured. The rate of infection among prisoners has fallen from 30 per cent to 7 per cent in 18 months.
Dr Sigurdur Olafsson, director of hepatology at Landspitali hospital in Reykjavik, believes there is "no question" Ireland and other countries can learn from the Icelandic experience. "It just takes collaboration. First you need to test – if you don't look for the disease, you won't find it."
The road to successful treatment is “long and tortuous with many bumps along the way”, he cautions, as patient drop out or get reinfected.
"Effectively what we're doing here is offering medication as vaccination," says Icelandic Health Authority ceo, Maria Heimisdottir. "So even if you have an unhealthy lifestyle, you're using needles and you're practising risky sex, the chances of you becoming infected with hepatitis C is approaching zero if the prevalence of the disease is also approaching zero.
“We’re looking for a form of herd immunity, so the disease will no longer be spread.”

Free treatment
The Icelandic programme has been facilitated through the provision by US drug manufacturer Gilead of free treatment for patients identified as having hepatitis C. The Icelandic government stumped up extra funding for harm reduction measures and additional staff.
None of those involved has any regrets about investing in the health of patients who have addictions. “People here realise a penny spent today is a dollar saved in a relatively short time,” says Heimisdottir.
“This is a disease. Not being able to stick to the treatment plan is part of the disease. It’s not a choice you have as an addict, you’re just not able to stick to it.”
In addition, she says, treating for hepatitis C has resulted in a “halo effect” as marginalised patients benefit in other ways from coming into regular contact with the health system. Transplant teams are also starting to notice an improvement in the availability of livers as the prevalence of the disease declines.
* The Irish Times travelled to Iceland in September on a visit for European press organised by Gilead



















